Hypobaric Oxygen Control System | Ideal Tool for Modeling Altitude Sickness Animals
Mountain sickness is a syndrome that occurs when people move from plains to plateaus (areas above 3,000 meters above sea level, which have obvious biological effects on the body) or from low-altitude areas to higher-altitude areas due to incomplete or maladjusted adaptability to the low-oxygen environment. The cause of the disease is hypoxia caused by the low-oxygen environment on the plateau.

China boasts the world's highest plateau, the Qinghai-Tibet Plateau. Known as the "Roof of the World" and the "Third Pole of the Earth," the plateau boasts an average elevation of 4,000 meters and accounts for 26% of my country's total land area. The harsh living environment, characterized by high altitude, oxygen deprivation, dryness, and strong ultraviolet rays, has left over 10 million people suffering from a variety of acute and chronic illnesses caused by hypoxia.
Classification of altitude sickness
Acute mountain sickness refers to the acute hypoxia reaction or disease that occurs when first entering the plateau. It is divided into: cerebral acute mountain sickness (also known as plateau coma or high-altitude cerebral edema), pulmonary acute mountain sickness (also known as high-altitude pulmonary edema), and mixed type (that is, the combined manifestation of pulmonary and cerebral types).Chronic mountain sickness refers to those who develop the disease more than half a year after arriving at the plateau or whose original acute mountain sickness symptoms persist. It is divided into: plateau heart disease, high-altitude polycythemia, high-altitude blood pressure abnormalities (including high-altitude hypertension and high-altitude hypotension), and mixed chronic mountain sickness (that is, heart disease and polycythemia coexist).
Among them, high-altitude pulmonary edema, high-altitude cerebral edema and high-altitude heart disease are the most serious symptoms of altitude sickness.
Current status of research on plateau diseases in my country
Driven by the national strategic goal of "expanding life space, developing western resources, ensuring national security, and promoting overall development," my country's plateau medicine research system has been gradually strengthened in recent years. This system has formed a working mechanism based on the prevention and treatment needs of altitude sickness, plateau diseases, infectious diseases, and endemic diseases, guided by clinical applications, centered around medical institutions, and supported by collaborative networks. This system has achieved positive results in basic research, academic exchange, talent development, and the application of research results.
In the field of high-altitude medicine, the study of altitude sickness has long been a focus of scientific attention. To better understand the pathogenesis of altitude sickness and explore effective prevention and treatment strategies, the development of accurate and stable animal models is crucial. This article will introduce several common methods for establishing animal models of altitude sickness.
Methods for establishing common animal models of altitude sickness
High Altitude Pulmonary Edema (HAPE) Model

High-altitude pulmonary edema (HAPE) is a severe, acute high-altitude disease characterized by rapid onset and progression, often occurring at night during sleep. Without timely diagnosis and treatment, it can be life-threatening.
Environmental simulation: SD rats were placed in a hypobaric oxygen chamber group (simulating hypoxia exposure at an altitude of 6000 m for 48 h) and a field hypoxia group (simulating hypoxia exposure at an altitude of 4200 m for 28 days);
Index detection: The dry-to-wet ratio, morphological and pathophysiological characteristics, expression of key genes aquaporin 1 (AQP-1) and vascular endothelial growth factor (VEGF), and oxidative stress levels of the lung tissue of experimental rats were detected;
Modeling Effect: Test results showed that pulmonary artery pressure and lung tissue water content increased significantly in both the hypobaric oxygen chamber and field hypoxia groups, while oxygen partial pressure and oxygen saturation decreased. Light microscopy revealed significantly widened alveolar walls and alveolar septa in both groups, with numerous red blood cells and inflammatory cells overflowing, and significant edema in the alveolar septa.
A hypobaric oxygen chamber simulates hypoxia exposure at an altitude of 6000 m for 48 h and can effectively establish a high-altitude pulmonary edema model in SD rats.
High Altitude Cerebral Edema (HACE) Model

Environmental simulation: Mice were placed in a hypobaric oxygen chamber to simulate an altitude of 6000m for 6h, 12h, 24h, 48h, and 72h.
Index detection: Brain edema was detected by weighing, blood-brain barrier (BBB) permeability was detected by Evans blue (EB), and cell apoptosis was detected by immunofluorescence staining;
Modeling results: The mortality rate of mice at an altitude of 6000 m was 12.2%. The HACE model established at an altitude of 6000 m exhibited brain cell enlargement and swelling, particularly at 24, 48, and 72 hours. Cells also showed disorganized arrangement, increased interstitial space, and nuclear condensation. Model validation revealed that brain edema and EB permeability increased after 12 hours in the HACE model mice established at an altitude of 6000 m, with no significant apoptosis at any time point.
A hypobaric hypoxic chamber simulating an altitude of 6000m (air pressure 47.19kPa, oxygen partial pressure 9.73kPa) for 48h can effectively establish a HACE model.
High Altitude Heart Disease (HAHD) Model

Environmental simulation: A low-pressure and low-oxygen animal experimental chamber was used to simulate the low-oxygen and low-pressure environment at an altitude of 6000m, with exposure for 1, 3, and 5 days respectively;
Tissue examination: HE staining results showed that hypoxia and hypobaric conditions caused varying degrees of damage to rat heart tissue, and the damage to myocardial tissue worsened with prolonged exposure under the above experimental conditions.
Index detection: The malondialdehyde (MDA) content and lactic acid (LD) content of myocardial tissue in each group increased significantly over time, while the reduced glutathione (GSH) content, total superoxide dismutase (T-SOD), and Na+ K+-ATPase activity decreased significantly over time;
Modeling effect: The simulated plateau environment of 6000m above sea level caused significant damage to the rat heart tissue, and the degree of damage was related to the time of exposure to hypoxia and low pressure. Reduced antioxidant capacity, increased free radicals and energy metabolism disorders were important factors leading to the damage.
A hypobaric oxygen chamber simulates hypoxic exposure at an altitude of 6000 m for 72 h and can effectively establish a high-altitude heart disease model in rats.
Molding equipment
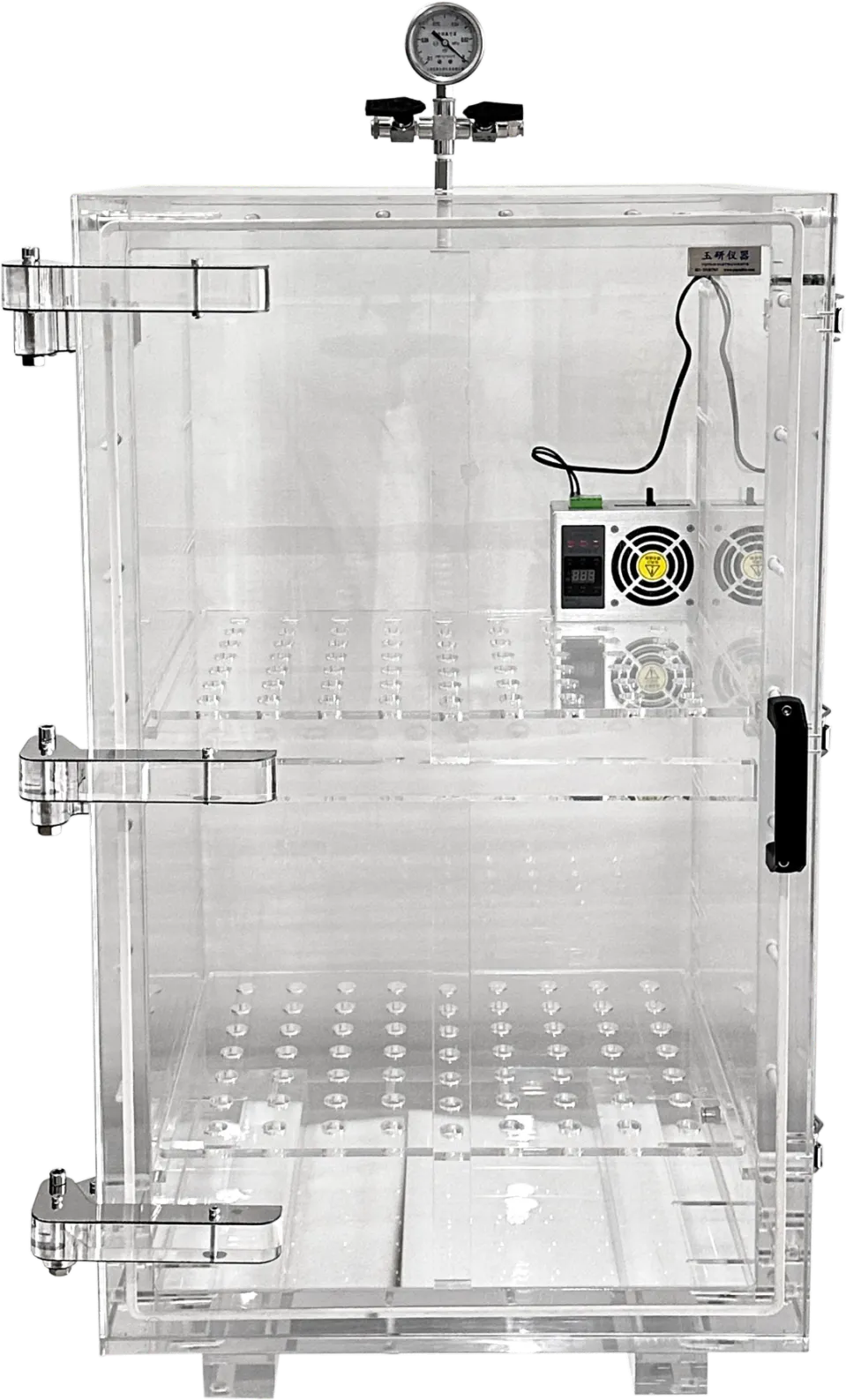
The Hypobaric Oxygen Concentration Control System utilizes the low-pressure, hypoxic environment of high altitudes to simulate the hypoxic environment found at high altitudes. This system can simulate the varying pressures at different altitudes, more accurately simulating the effects of varying altitudes on experimental animals.Shanghai Yuyan Instruments' independently developed low-pressure oxygen concentration control system has been widely acclaimed and deployed in numerous domestic laboratories. The instrument's fully transparent acrylic enclosure offers a sturdy, airtight seal, ensuring constant pressure and facilitating observation of the animal's vital signs and activity. The system can simulate low-pressure oxygen environments at altitudes ranging from 0 to 10,000 meters.

Low-pressure oxygen concentration control system
Meet a variety of research needs:
Effects of hypobaric hypoxia on water content and oxygen saturation in rat lung tissue; Effects of hypobaric hypoxia on adenosine nucleotide content and energy charge in rat brain mitochondria; Effects of hypobaric hypoxia on the degree of myocardial tissue damage in rats.
And various other scientific studies related to low pressure, such as the effects of low-pressure hypoxia on the kidney function and structure of rats, drugs for treating altitude sickness, etc.
Technical Principle
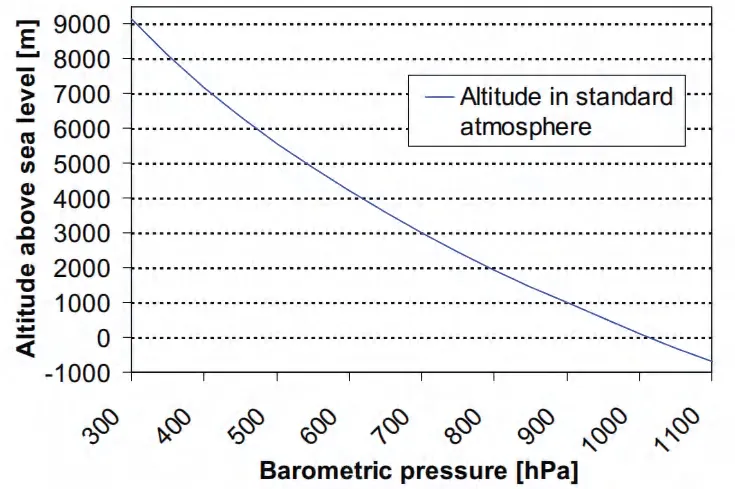
A low-pressure environment reduces the total air pressure, thereby reducing the partial pressure of oxygen in the air, resulting in a decrease in the amount of oxygen inhaled.
In a gas mixture (such as air), the partial pressure of each gas refers to the pressure it occupies in the mixture. The total pressure is equal to the sum of the partial pressures of all gases. At high altitudes or in low-pressure environments, the total pressure decreases. Since the proportion of oxygen in air remains constant (approximately 21%), the oxygen partial pressure decreases accordingly. The amount of oxygen inhaled by the human body or other organisms is directly proportional to the oxygen partial pressure of the inhaled gas. Therefore, in a low-pressure environment, although the volume fraction of oxygen in the air remains unchanged, the lower oxygen partial pressure reduces the number of oxygen molecules inhaled, resulting in an insufficient oxygen supply.
Therefore, by controlling the air pressure value inside the instrument and controlling parameters such as the temperature and humidity of the environment inside the low-pressure oxygen chamber, low-pressure and oxygen-deficient environments at different altitudes can be simulated.
The low-pressure oxygen concentration control system mainly consists of three parts: the main unit, the low-pressure oxygen chamber and the gas circuit controller.
(1) Main unit - precise pressure control
The host uses a feedback design pressure controller to ensure that the pressure in the cabin is maintained within the target range, and can simulate a maximum altitude pressure of 10,000m.

(2) Hypobaric oxygen chamber - transparent box for easy observation
Provide a stable and continuous breeding environment. During the experiment, the animals can be placed in a breeding cage (with food and water) and placed in a low-pressure chamber. The animals can live in the chamber for a long time.
(3) Gas circuit controller - regulates and controls the exchange of gas, intermittently introduces fresh gas to maintain fresh air in the cabin and avoid excessive temperature inside the cabin. The on/off time ratio can be customized.

Precise pressure control: with a pressure feedback mechanism, it can detect and control the air pressure in the cabin in real time, and maintain the set pressure range in the oxygen chamber for a long time. Transparent cabin material: the oxygen chamber is made of transparent acrylic, which can observe the status of the animals at all times. Support for long-term experiments: equipped with a circulating ventilation system to provide fresh gas to the low-pressure oxygen chamber while maintaining the dynamic balance of pressure in the cabin. Layered cabin design: a partition is set inside the oxygen cabin to achieve two layers, which can simultaneously separate 2 rat cages or 6 mouse cages. Strong scalability: a humidity controller can be added to strictly control the humidity of the oxygen chamber environment; an optional pressure gradient rise control module can be used to control the gradient rise time of the simulated altitude, giving animals more time to adapt. Flexible operation: screen button settings, one-click start
Application Cases
High altitude heart disease (HAHD) is a complex pathophysiological condition associated with systemic hypobaric hypoxia caused by altitude sickness. Hypoxia can lead to myocardial metabolic disorders, increasing the risk of heart failure and sudden cardiac death. Aldehyde dehydrogenase 2 (ALDH2) regulates myocardial energy metabolism and plays a protective role in various cardiovascular diseases.
The article "Aldehyde dehydrogenase 2 serves as a key cardiometabolic adaptation regulator inresponse to plateau hypoxia in mice" published by Rifeng Gao et al. in Translational Research aimed to determine the effects of high-altitude hypoxia (PH) on cardiac metabolism and function, explore the related roles of ALDH2, and explore potential therapeutic targets.
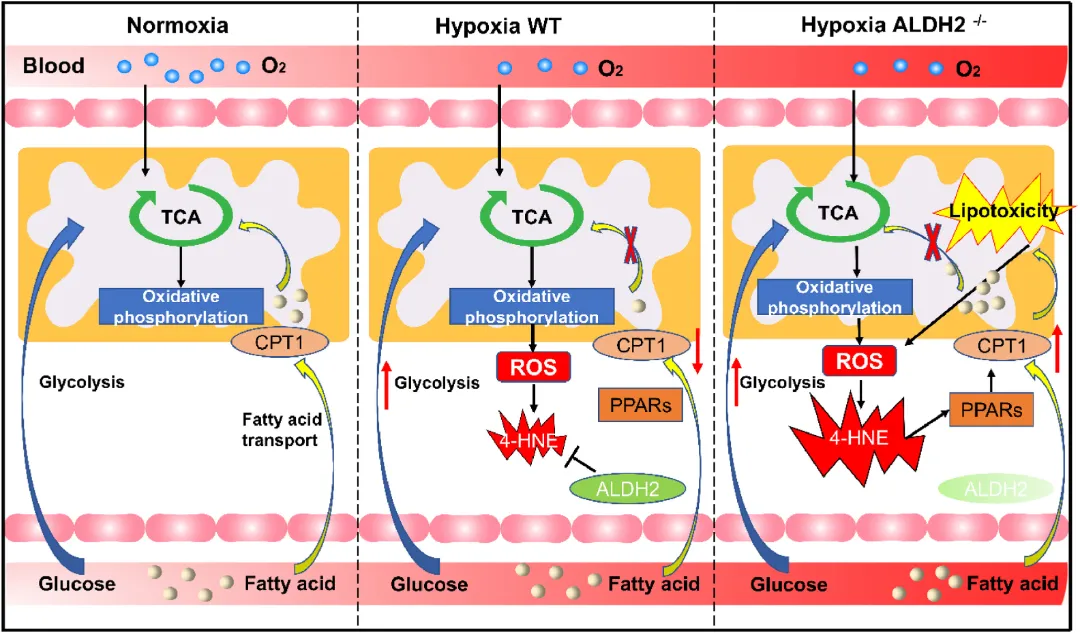
The authors found that PH significantly reduced animal survival and cardiac function, and ALDH2 deficiency exacerbated these effects. PH also led to a shift in myocardial energy sources from fatty acids to glucose, and ALDH2 deficiency impaired this adaptive metabolic shift. Untargeted and targeted metabolomics and transmission electron microscopy revealed that ALDH2 deficiency promoted myocardial fatty acid deposition, leading to enhanced fatty acid transport, lipotoxicity, and mitochondrial dysfunction.
In addition, experimental results showed that ALDH2 attenuated PH-induced adaptive metabolic program damage through the 4-HNE/CPT1 signaling pathway, and the CPT1 inhibitor etomoxifloxacin significantly improved the heart damage induced by ALDH2 deficiency in PH mice and increased the survival rate of PH mice.
In conclusion, our data suggest that ALDH2 is a key regulator of cardiometabolic adaptations in response to PH. The CPT1 inhibitor etomoxifloxacin may attenuate the effects induced by ALDH2 deficiency and improve cardiac function in response to PH.
In this paper, a low-pressure oxygen concentration control system provided by Shanghai Yuyan Scientific Instrument Co., Ltd. was used to establish a plateau hypoxia (PH) model to simulate high altitude heart disease (HAHD).
The specific method was to house mice in a simulated high-altitude environment (6000 m, 47.2 kPa atmospheric pressure, 11.35% O₂) for 2 weeks. The airflow within the oxygen chamber was 2 L/min, and the relative humidity was maintained at 50-55%. Every 24 hours, the animals were removed from the hypobaric oxygen chamber for 15 minutes to replenish food and water. The experimental animals were maintained under a 12-hour light/dark cycle.
The CPT1 inhibitor etomoxifloxacin (1 mg/kg) was administered intraperitoneally every three days for two weeks before and after hypobaric oxygenation. Myocardial tissue was isolated from the mice two weeks later and subjected to single-cell analysis of myocardial contractile and diastolic function, measurement of reactive oxygen species, ATP detection, determination of ALDH2 enzyme activity, metabolomics analysis of medium- and long-chain fatty acids, mitochondrial isolation and assessment of mitochondrial complex activity, and analysis of cardiomyocyte oxygen consumption (OCR).
Partial user list